HIPAA-Compliant ITSM: What Healthcare IT Teams Actually Need
Category
Service Management
Uncategorized
.svg)
Category
HIPAA-compliant ITSM means your IT service management platform can execute a Business Associate Agreement (BAA), maintain auditable trails on every ticket that touches protected health information, enforce role-based access by clinical role, and support breach notification workflows, not just encrypt data in transit. If your current ITSM vendor can't check all four boxes, you have a compliance gap, regardless of what their security page says.
I spent a decade inside the ServiceNow ecosystem, 400+ deployments, and I was the partner that brought ServiceNow to the Australian market. I know what enterprise-grade ITSM looks like. I also know why a 600-bed regional hospital has no business paying for it, and no realistic path to running it without a team of consultants. That's the gap Servicely was built for. And healthcare is where that gap is most dangerous.
This post breaks down what HIPAA compliance actually requires from your ITSM platform, why the two most obvious options (ServiceNow and Freshservice) both fail mid-market healthcare IT teams for different reasons, and what you should actually be looking for before you sign anything.
Most IT teams manage productivity tools, laptops, and enterprise applications. Healthcare IT teams manage all of that, plus the clinical infrastructure that keeps patients alive.
When your hospital's EHR goes down, that's not a productivity issue. It's a patient safety event. Clinicians fall back on paper processes, medication orders slow down, and lab results get delayed. The stakes on every P1 incident are categorically different from what an IT team at a logistics company or a SaaS business faces.
That changes what you need from your ITSM platform in specific, practical ways.
This is where most ITSM vendors handwave. Let's be specific about what compliance actually requires.
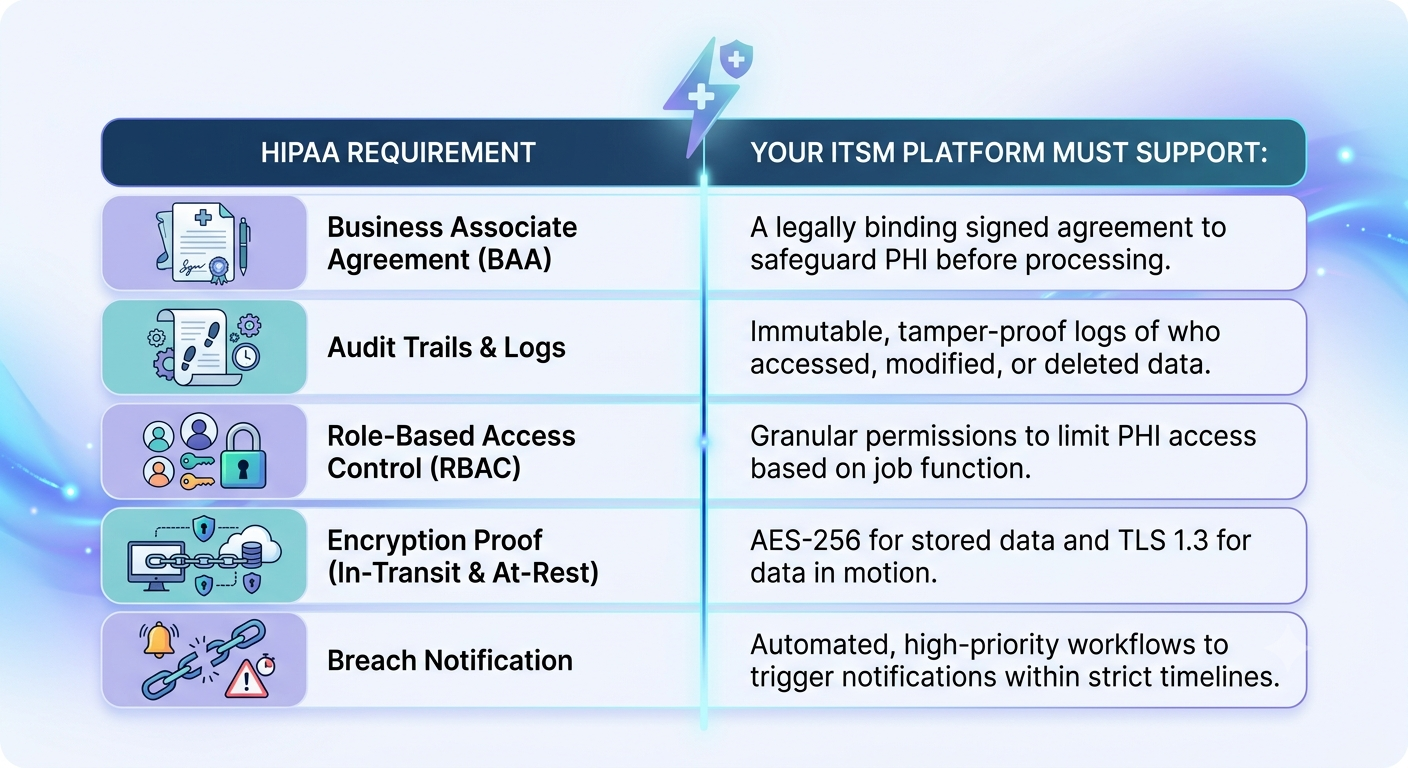
There's a widespread misconception that "HIPAA-compliant" is a certification you get from a third party. It's not. There's no HIPAA certification body. HIPAA compliance is an ongoing operational posture, and for your ITSM platform, it comes down to five non-negotiable requirements.
If your ITSM vendor handles ePHI on your behalf and won't sign a BAA, they are not a business associate; they're a liability. The BAA establishes that the vendor is contractually bound to comply with HIPAA's safeguard requirements and is responsible for violations that occur on its infrastructure. Without it, your organization absorbs the full risk.
Not every ITSM vendor will sign a BAA. Some won't because they haven't invested in the compliance infrastructure to support it. Ask directly, before any other conversation: "Will you sign a BAA with us?" If the answer is anything other than a clear yes, stop the evaluation.
HIPAA's Security Rule requires that you can account for every access to ePHI, who accessed it, when, from what system, and what they did. In an ITSM context, that means: who created the ticket, who viewed it, who modified it, who reassigned it, and when each of those actions happened. Those logs must be immutable, exportable for audits, and retained for a minimum of six years.
Many ITSM platforms log ticket changes but don't log ticket views. That's a gap. If an unauthorized employee looks at a ticket containing ePHI and there's no view log, you can't demonstrate that access was appropriate during an OCR audit.
Not everyone in your organization should be able to see every ticket. In healthcare, this means your ITSM must support access tiers that map to clinical roles: ICU staff, administrative staff, facilities management, and IT staff all have different legitimate access needs. A ticket about a malfunctioning infusion pump in the oncology ward shouldn't be visible to the front desk coordinator.
Your ITSM platform needs RBAC that's granular enough to enforce this without requiring a developer to configure it every time you add a new role or department. If your current system can't do this without custom development, you're running on compliance debt.
AES-256 encryption at rest and TLS 1.2+ in transit are now the floor, not a differentiator. But ask your vendor for the documentation, not just their word. Where is your data hosted? Is it AWS, Azure, or a third-party data center? What's their SOC 2 Type II status? If they can't produce audit documentation, "encrypted" is a marketing word, not a compliance posture.
Under HIPAA, you have 60 days to notify affected individuals and HHS after discovering a breach involving 500 or more records. If your ITSM platform doesn't support incident classification workflows that can identify a potential ePHI breach, route it to your privacy officer, document the investigation steps, and trigger notification workflows, you're managing your breach response in email threads and spreadsheets. That's not a system of record; that's a liability.
The civil monetary penalties for HIPAA violations in 2026 range from $145 per violation (for cases where the covered entity didn't know) up to $2,190,294 per violation for willful neglect that isn't corrected, according to current HHS penalty schedules. "We didn't have the right ITSM workflows" is not a defense that reduces penalties.
ServiceNow is a serious platform. I'm not going to pretend otherwise; I spent a decade deploying it. Half of the top 40 US healthcare providers use it. For a system like Kaiser Permanente or Cleveland Clinic with a large in-house ServiceNow team, centralized procurement leverage, and multi-year implementation timelines, ServiceNow makes sense.
For a 600-bed regional hospital, it doesn't. Here's why.
The pricing reality. A typical ServiceNow ITSM deployment for a mid-market organization, let's say 50 fulfillers, runs $150K to $400K annually in license fees, depending on module selection and negotiation. But the license is only part of the cost. Implementation fees typically eclipse your annual license cost by 3 to 5 times. When you sign a $200K ServiceNow license agreement, your true first-year total cost of ownership is between $800K and $1.2M when you factor in implementation consulting, customization, data migration, and change management.
We've seen this directly with customers who came to us. One organization was paying $562K annually for ServiceNow for equivalent module coverage that Servicely delivered for $120K, a 73% platform cost reduction. That $440K gap is real budget that could go to clinical staff, equipment, or infrastructure.
The consultant dependency. Every time you need to change a workflow in ServiceNow, you need a certified ServiceNow developer or a consulting engagement. There's no realistic self-service administration for a mid-market IT team. When your VP of IT is also your ServiceNow admin, which is the reality at most 500-2,000-employee hospitals, every change request becomes a project with a statement of work and an invoice.
The implementation timeline. ServiceNow implementations take 6 to 12 months for a properly scoped deployment. A mid-market hospital IT team doesn't have 6 to 12 months of implementation overhead on top of their day jobs managing clinical uptime. The implementation project itself becomes a crisis rather than a solution.
For more on the real cost comparison, see our full ServiceNow vs Servicely breakdown , including a module-by-module pricing table we don't publish anywhere else.
Freshservice, Zendesk, and Jira Service Management are good products for specific use cases. If you're running a 50-person startup that needs a basic helpdesk, Freshservice is probably the right choice. But they weren't built for healthcare IT, and the gaps show up when you need them most.
The BAA problem. Freshservice offers a BAA for its enterprise tiers. Zendesk offers one. But a BAA alone doesn't make a platform HIPAA-compliant; it just means the vendor accepts contractual responsibility. The underlying platform still needs the audit-trail depth, RBAC granularity, and breach-notification workflows required by HIPAA. A BAA from a vendor whose logging capability covers ticket changes but not ticket views is a legal document that creates false confidence.
Clinical workflow blindness. These platforms weren't designed with clinical priority tiers in mind. The difference between a P1 ticket (EHR down, clinical operations affected) and a P2 ticket (a single workstation with a broken keyboard) matters enormously in a hospital. Freshservice's priority framework is built around standard IT service tiers. Mapping it to clinical urgency is possible, but it requires configuration work that most mid-market healthcare IT teams don't have the bandwidth to do correctly.
SLA structures that don't reflect clinical operations. A standard Freshservice SLA assumes business hours. Healthcare IT doesn't have business hours. Configuring 24/7 SLA tiers, shift-based on-call routing, and clinical escalation paths in a platform that wasn't built for it is painful. It's the kind of thing that looks fine in a demo and breaks at 3 a.m. on a Tuesday.
No understanding of healthcare IT ticket patterns. An AI-native platform built for IT understands the difference between a password reset (automate), a network switch failure (escalate immediately with change management linkage), and an EHR interface going down (P1 with clinical impact, bridge to incident management). Customer support AI tools, which are what Freshservice's Freddy AI and Zendesk's AI started as, treat all tickets the same.
For a deeper look at how AI-native ITSM handles these distinctions, see our post on AI solutions for ITSM, specifically the section on ticket classification in regulated environments.
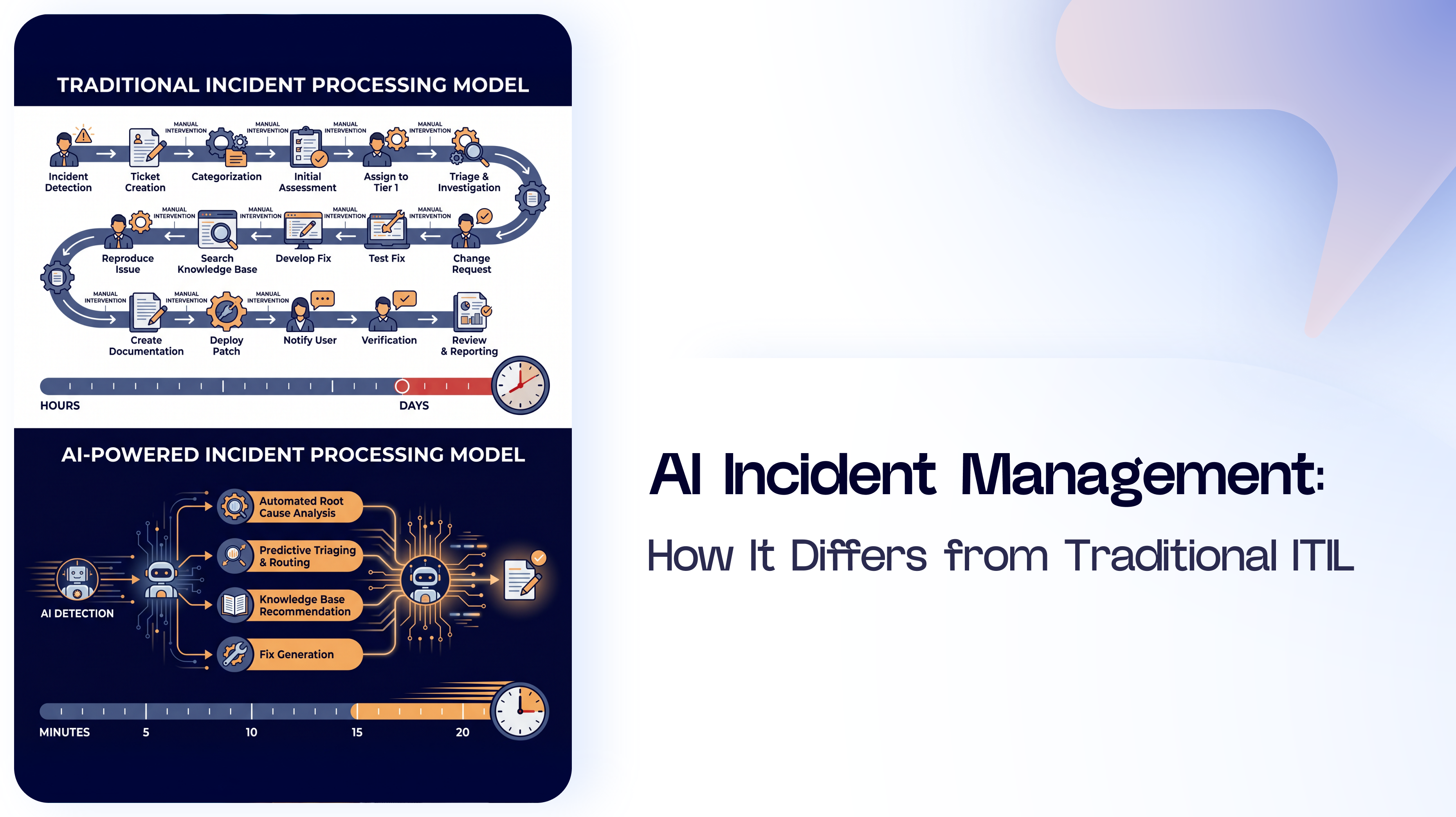
This is where the architectural difference between Servicely and traditional platforms becomes concrete rather than theoretical.
Automated password resets. Between 20% and 50% of all IT help desk tickets are password-related, according to HDI benchmarking. In healthcare, clinicians who move between shared workstations and multiple clinical applications increase this number. An AI-native ITSM platform can verify identity through multi-factor authentication and execute the reset without human intervention. That ticket never gets to a technician. It gets resolved in seconds.
For a 500-bed hospital IT team handling 300 tickets a day, if 100 of those are password resets and 80% can be auto-resolved, that's 80 technician-hours per day redirected from manual resets to clinical infrastructure work.
Clinical vs non-clinical ticket classification. Servicely's AI classifies tickets at the point of submission, not after a human has read them. A ticket logged as "can't access Epic" is immediately classified as a clinical EHR access issue, routed to the appropriate tier-2 queue with CMDB context, and flagged for clinical impact tracking. That routing happens in milliseconds. Manual triage takes 15-30 minutes per ticket.
Predictive device failure detection. With integration to your endpoint monitoring, AI-native ITSM can identify patterns across tickets that indicate a device class is failing before the calls flood in. If six clinical workstations in the same ward have generated similar error tickets in the last 72 hours, a problem record gets created proactively. In most hospitals, that correlation occurs during a post-incident review, not in a prevention workflow.
Knowledge article generation from resolved incidents. Every time a technician resolves a ticket, AI can draft a knowledge article from the resolution notes and propose it for publication. Over time, your knowledge base reflects how your specific environment actually fails, not generic vendor documentation. When the same issue recurs, the self-service portal surfaces the solution before the ticket gets submitted.
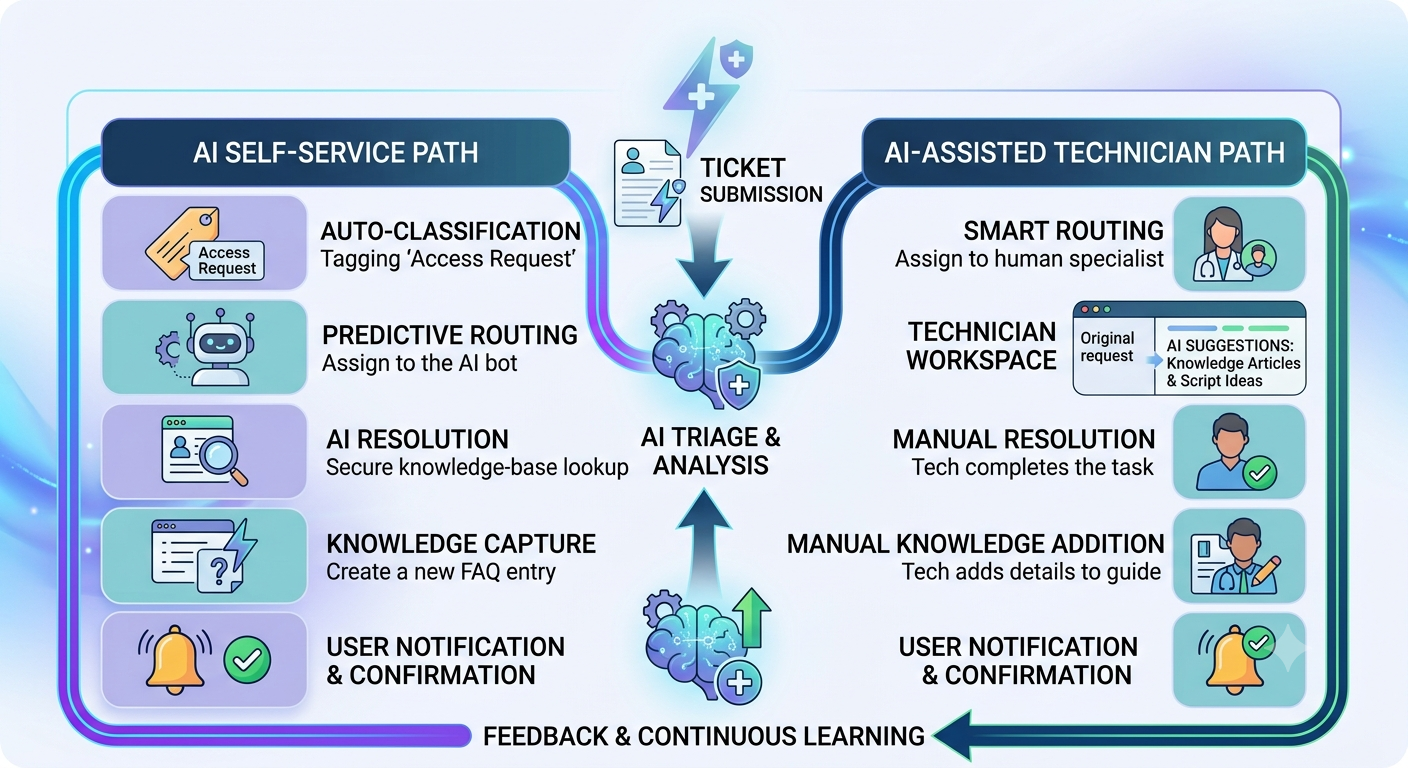
This is what AI-native means in practice. Not a chatbot bolted onto a 2010-era ticketing platform. AI running across every workflow from submission to resolution to knowledge capture.
For more on what ITSM self-service looks like with AI, see our self-service portal guide.
Before you sign a contract with any ITSM vendor, get definitive answers on each of these. Not marketing-page answers. Written answers from their legal and compliance team.
BAA and Compliance
Clinical Operations
AI and Automation
Commercial Reality
If a vendor can't answer yes to all of these, note the gaps before you negotiate. A "yes" on BAA but a "no" on audit log depth means the BAA is covering a platform that doesn't meet the underlying requirement.
See how Servicely handles healthcare IT service management , book a 30-minute demo tailored to your clinical workflow.
Mid-market healthcare IT is an underserved market. ServiceNow is too expensive and too complex. Freshservice and Zendesk weren't built for clinical environments. The few platforms that specialize in healthcare ITSM, Giva, and the healthcare-specific modules in ManageEngine lack the AI-native architecture that actually solves the operational problems: password reset volume, clinical ticket classification, and predictive device management.
The combination of HIPAA compliance requirements, genuine AI-native capability, and pricing that doesn't require a seven-figure IT budget is what mid-market hospitals actually need. That's not a comprehensive market. But it's the gap Servicely was built for.
If you're running healthcare IT at a hospital or health system with 500 to 5,000 employees, you're probably either overpaying for ServiceNow or under-supported on a lightweight platform. Either way, it's worth 30 minutes to see what a right-sized alternative looks like.
For a direct side-by-side comparison on pricing, implementation timelines, and HIPAA compliance features, see Servicely vs. ServiceNow.
Ready to see HIPAA-compliant ITSM in action? Request a demo

.png)






